IVUS imaging helps you decide, guide and confirm the right interventional treatment for each patient. IVUS-guided PCI strategies are backed by a wealth of clinical studies. The ESC gives a Class I, level of evidence A recommendation when performing PCI on anatomically complex lesions, in particular left main stem, true bifurcations, and long lesions.1 Explore the various studies below to learn more about the evidence that drove the ESC to give the highest level of recommendation in the guidelines.

ESC elevates intravascular imaging to a Class IA recommendation
Plug-and-play simplicity of Philips Eagle Eye Platinum is an easy way for physicians to get with the IVUS guidelines.
For this systematic review and updated meta-analysis, investigators searched the publication databases from inception through August 30, 2023, for studies that randomly assigned patients undergoing PCI with drug-eluting stents to either IVUS or OCT, or both, or to angiography alone to guide their interventions.
Meta analysis of 22 randomized controlled trials with nearly 16,000 patients reinforces the benefits of image-guided PCI. Imaging improves outcomes and saves lives.2
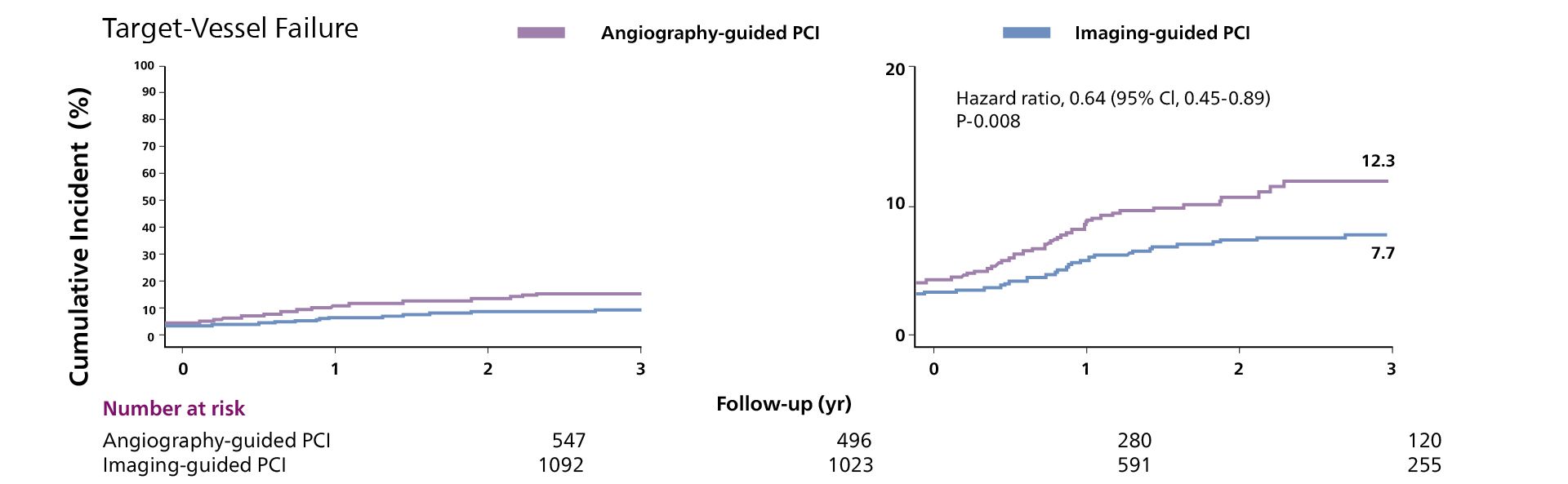
Intravascular image–guided PCI with IVUS or OCT versus angiography-guided PCI in patients with complex coronary-artery lesions
Intravascular image-guided PCI was associated with a lower incidence of a composite of cardiac death, target vessel-related myocardial infarction, or clinically driven target vessel revascularization compared to angiography guided PCI.3
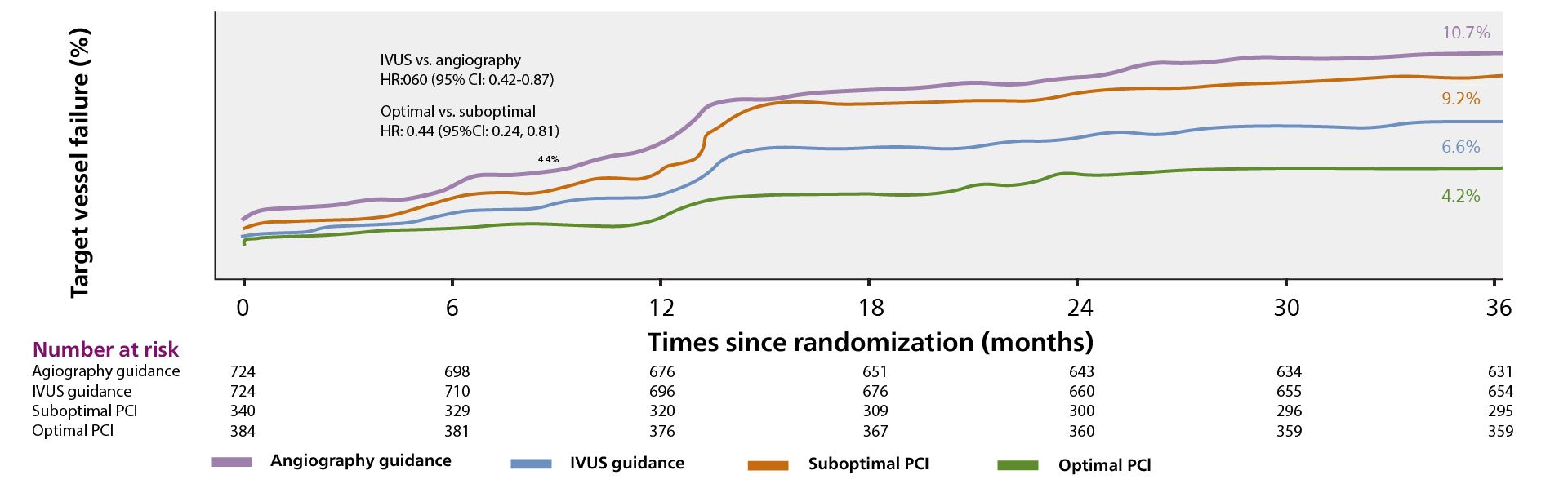
IVUS-guided DES implantation was associated with significantly lower rates of target vessel failure and stent thrombosis during a 3-year follow-up among all comers, particularly those who underwent the IVUS-defined optimal
Compared to angiography-guided PCI alone, in all comer patients, ULTIMATE shows that IVUS-guided PCI significantly reduces Target Vessel Failure (TVF) mainly driven by the decrease in clinically driven target vessel revascularization (TVR). This benefit was sustained over three years. Only 1.6% TVF at 12 months and 4.2% TVF at 3 years when optimal IVUS-guided PCI criteria was met.
Primary endpoint based on patient-level comparison
The ADAPT-DES study reported that IVUS guidance was associated with:
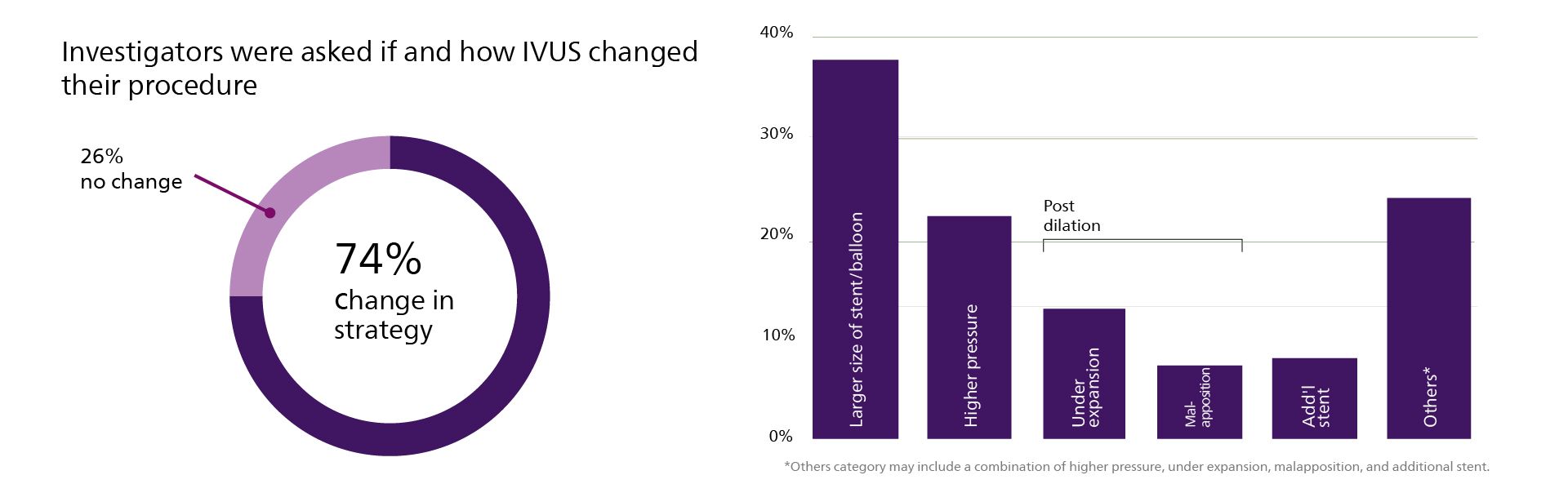
Guidance strengthens use of IVUS during stent implantation and to determine the mechanism of stent restenosis and thrombosis.8
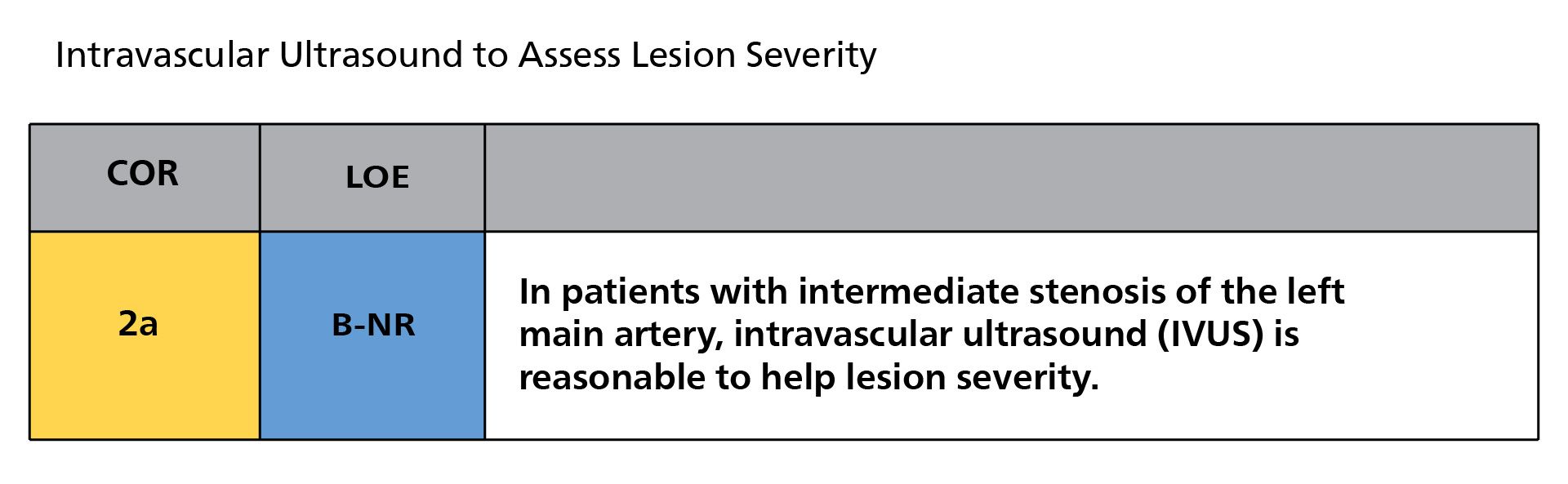
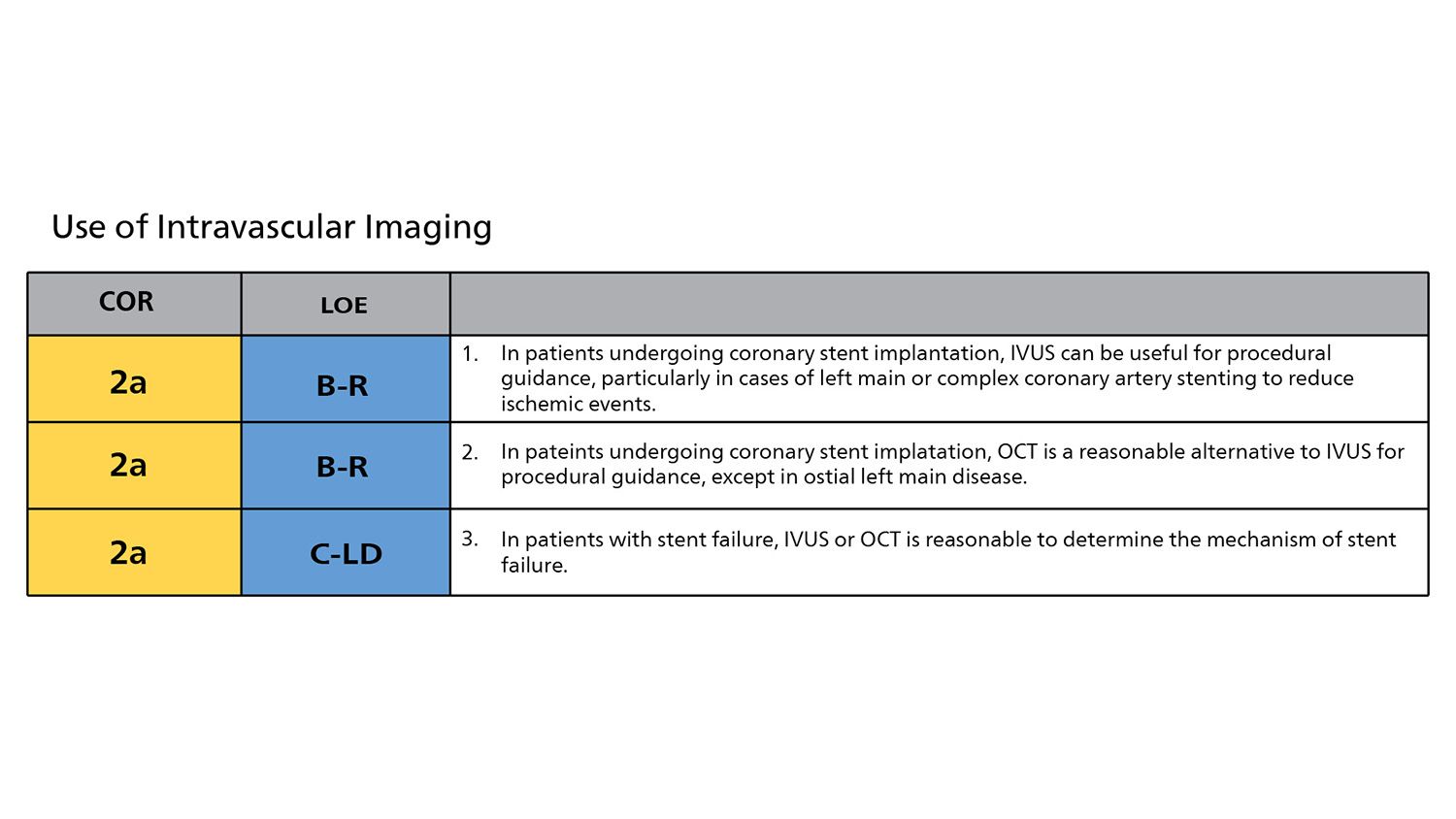
All 2B recommendations from the 2011 guidance elevated to 2A in 2021 guidelines.
